


News
Surgical robots are Not New. Intelligent Ones are
Date: Apr 01 2026
Publication: Analyticsindiamag.com
For more than a decade, robotic systems have been a fixture in advanced operating rooms, enabling surgeons to perform minimally invasive procedures with greater precision and control.
Platforms such as the da Vinci Surgical System allow doctors to translate hand movements into fine, tremor-free actions, reducing complications and improving recovery times. However, these systems primarily execute commands without understanding context.
At Tata Elxsi, teams are developing AI systems that analyse live surgical video feeds to identify anatomical structures and assist surgeons during procedures. “The robot, as it stands today, is largely an execution system,” Anup SS, Practice Head of Artificial Intelligence and Machine Learning, explains in conversation with AIM. “What AI brings in is the ability to interpret what is happening during the surgery and provide additional awareness to the surgeon.”

In minimally invasive procedures such as gallbladder removal, surgeons operate via a camera view, navigating tight anatomical spaces where even small deviations can lead to complications. AI models trained on surgical data can highlight organs and critical structures in real time, helping surgeons avoid unintended damage. “If you are operating very close to a critical structure, the system can alert you,” Anup said. “That additional layer of information can make a significant difference.”
While robotic systems address challenges such as hand stability and access, they do not eliminate the need for continuous interpretation. Surgeons must still assess visual information, anticipate risks, and make decisions under pressure. AI introduces a second layer of analysis. “These systems can act as an additional set of eyes,” Anup says. “They can continuously monitor what is happening and bring out details that may not be immediately obvious.”
Quantifying injury
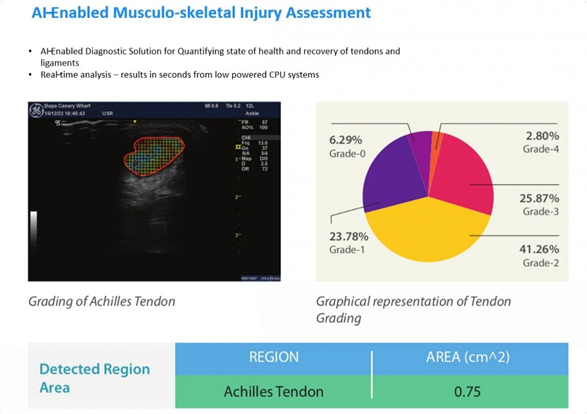
The image shows an AI-enabled system designed to assess musculoskeletal injuries, specifically focusing on the Achilles tendon using ultrasound imaging. The system identifies the tendon region and maps the extent of injury using colour-coded segmentation, where different colours indicate varying levels of damage.
“This is something that is very difficult to assess visually in a consistent way,” Anup explains. “Different doctors may interpret the same scan differently, especially when the injury is not clearly demarcated.”
Alongside the image, a graphical breakdown quantifies the severity of the injury across different grades, offering a percentage-based distribution. This allows clinicians to move beyond visual assessment and rely on measurable data. The system also calculates the affected area, helping to standardise evaluation.
“With AI, we can quantify the extent of injury and track it over time,” he added. “If the numbers are improving, the treatment is working. If not, the approach needs to be changed.”
Such tools, he notes, are particularly useful in monitoring recovery, where subtle improvements may not be immediately visible through manual observation.
In practical terms, this could include identifying anatomical boundaries, detecting abnormal patterns, or flagging proximity to sensitive areas during surgery. In some cases, AI models are also being developed to assess intraoperative risks such as blood flow. “If there is an abnormal flow, the system can estimate the severity and alert the surgeon,” he adds.
“Our customers span hospitals like Aster, global device manufacturers, and clinical research bodies. In healthcare, you need an ecosystem to build meaningful AI solutions,” Anup said.
AI’s role in surgery reflects a broader shift across healthcare, particularly in diagnostics and imaging, where it helps analyse scans in near real time and reduce reporting delays. “A CT scan may be done in 20 minutes, but the report may come only the next day because the radiologist has a queue. AI can help reduce that delay significantly,” Anup points out. It is also enabling early screening of conditions like glaucoma and improving hospital workflows by easing the burden on technicians.
Despite its potential, AI in healthcare faces challenges, particularly around data quality and model reliability. “Public datasets are available in large volumes, but their quality may not always be adequate,” Anup says. “In many cases, we have to re-annotate and validate the data before it can be used.”
Ensuring that models generalise well is another critical requirement. According to him, it is important that the system is trained on one dataset and tested on a completely different dataset. Only then can one assess whether it is truly reliable.
Even with such safeguards, limitations remain. “No AI model is 100% accurate,” Anup says. “In healthcare, we design systems to ensure that no case is missed, even if that means accepting a small percentage of false positives.”
Acknowledging the concern, Anup cites a case in which an AI-generated report introduced an incorrect diagnosis. “The system added a condition that was not identified by the doctor, and it went through without being noticed.”
Such incidents highlight the need for human oversight. “The AI system should assist, but the final decision must always be with the doctor,” he says. “Clinical correlation is essential.”
While individual use cases—from surgical assistance to diagnostics—are advancing, fully integrated AI-driven healthcare systems are still in development. “Today, many of these capabilities exist in silos,” Anup said. “The real value will come when they are brought together into a single ecosystem.”
This would involve integrating pre-operative imaging, intraoperative guidance, and post-operative monitoring into a unified framework, enabling more consistent, data-driven care.
The introduction of AI into surgical environments does not fundamentally change the surgeon’s role. “The idea is not to replace the doctor, but to provide better tools,” Anup says. “If we can bring more information to the surgeon at the right time, it can improve outcomes.”
In that sense, the evolution of surgical robotics is less about disruption and more about augmentation.